
Jul 30
Jul 30
Jul 29
Jul 22
Jul 19
Jul 17
Braces make great smiles—but they also trap plaque, test your patience, and can irritate gums. A gentle electric toothbrush solves the puzzle: sonic power for deep cleaning, smart pressure control to protect tissue, and app guidance so you don’t miss a spot. Here’s a braces-friendly routine with BrushO to keep teeth, gums, and brackets happy. 🦷✨
Brackets and wires create tiny hideouts for food and bacteria 🦠. Scrubbing harder won’t fix it—overbrushing risks enamel wear and gum recession. What you need is precise, low-pressure cleaning that reaches around hardware without stressing your mouth.
A gentle electric toothbrush does the heavy lifting with micro-vibrations, not elbow grease.
BrushO Smart Electric Toothbrush combines comfort with control:
🌸 Gentle & Gum-Care modes — soothing on tissue, effective on plaque
📳 Smart pressure sensor — nudges you to ease up before gums get irritated
🌊 Sonic micro-vibrations — help dislodge buildup around brackets and between teeth
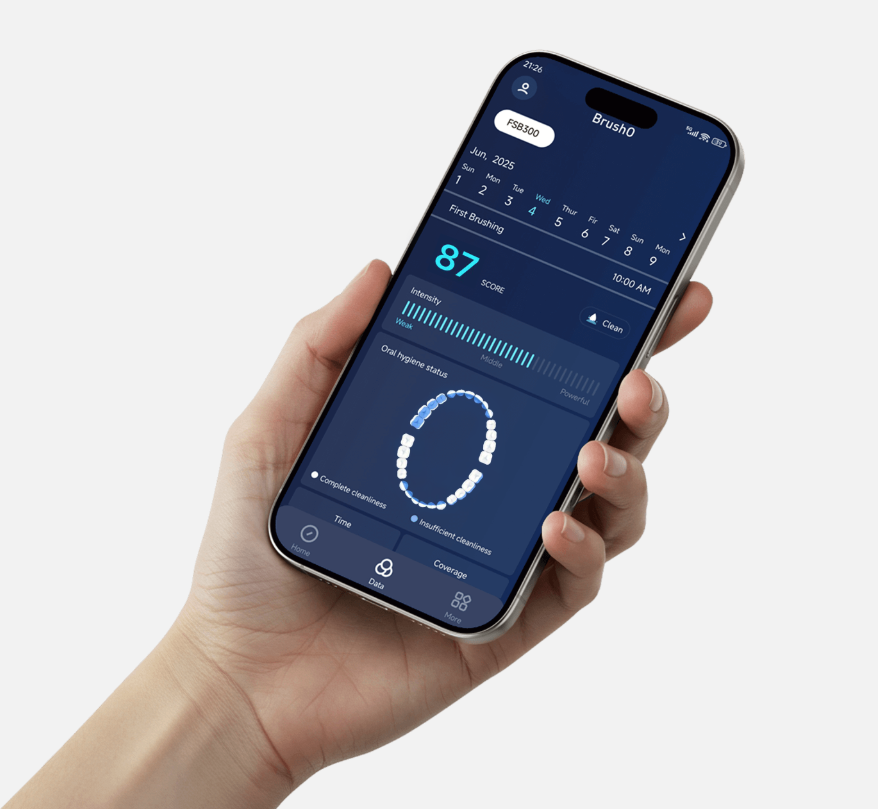
📱 App guidance — real-time coverage feedback so no quadrant gets ignored
🔋 Travel-ready battery — up to ~45 days per full 6-hour charge (perfect for school trips)
🚿 IPX7 waterproof — brush at the sink or in the shower with confidence
1. Pick Gentle or Gum-Care mode. Start soft; let sonic power do the work.
2. Angle 45° to the gumline. Glide, don’t scrub. Short, slow passes win.
3. Above the bracket → on the bracket → below the bracket. Think of it as a three-lane sweep for each tooth.
4. Trace the wire. Tilt the brush to clean where plaque likes to hide.
5. Sweep behind front teeth. Use the tip to clean the lingual surfaces.
6. Finish with tongue & cheeks. Quick pass for fresher breath. 😮💨
7. Check coverage in the app. Fill the map; aim for 100% over time.
⏱️ Timing tip: 2 minutes, twice a day. Add 30–60 seconds at night for bracket detail work.
Morning (2–3 min)
Evening (3–4 min)
Weekly add-ons
Quick FAQ for Brace-Wearers ❓
Is an electric brush safe with braces?
Yes—choose gentle modes and pressure control to protect tissue and hardware.
Which bristles should I use?
Soft, rounded bristles are kinder to enamel and gum margins.
How long should I brush?
At least 2 minutes (AM/PM). Add focused bracket passes at night.
Do I still need interdental cleaning?
Absolutely. Your brush handles surfaces; floss/interdental tools handle in-between
Braces demand precision, not force. With BrushO’s gentle modes, sonic power, pressure sensing, and app coaching, you’ll clean more thoroughly, protect your gums, and keep brackets spotless—without the aches and guesswork.
🛒 Ready for brace-friendly brushing?
👉 Get the BrushO Gentle Electric Toothbrush
Jul 30
Jul 30
Jul 29
Jul 22
Jul 19
Jul 17

Tooth eruption is the process by which a tooth moves from its developmental position within the jawbone to its functional position in the oral cavity. It is a precisely timed, multi-stage journey that involves the coordinated action of the dental follicle, the periodontal ligament, and the surrounding alveolar bone. The permanent tooth must navigate through millimeters of bone, avoid adjacent tooth roots, and time its arrival to coincide with the exfoliation of the overlying primary tooth.

Every time you consume fermentable carbohydrates, the pH at the tooth surface plummets from a neutral 7.0 to a critical 5.5 or below within minutes, initiating enamel demineralization. This acid attack — described by the Stephan curve — can last 30 to 60 minutes, during which saliva's bicarbonate, phosphate, and urea buffering systems work continuously to neutralize acids and restore the mouth to a safe pH. Understanding this cycle is the biochemical foundation of caries prevention.

Periodontal pockets — the pathological deepening of the gingival sulcus beyond 3 mm — develop silently over months and years, driven by a bacterial biofilm that triggers a destructive host inflammatory response. Once formed, these pockets become self-sustaining reservoirs of anaerobic pathogens that progressively destroy the periodontal ligament and alveolar bone, making them the primary anatomical driver of adult tooth loss.

When nasal airflow is compromised, the switch to mouth breathing triggers a cascade of oral physiological changes that begin within weeks. The constant evaporation of saliva dries the oral mucosa, reduces the pH-buffering capacity that protects enamel from acid erosion, and inflames the anterior gingiva, which is no longer bathed in the protective, humidifying envelope of lip seal. The result is accelerated enamel demineralization, increased caries risk, and a distinctive pattern of anterior marginal gingivitis.

The ulcerated pocket epithelium that lines a periodontal pocket is not just a site of local inflammation — it is a breach in the body's mucosal barrier that allows oral bacteria direct entry into the systemic circulation. Every act of chewing, brushing, or even swallowing can propel billions of periodontal pathogens into the bloodstream, where they can seed distant organs including the heart, brain, liver, and placenta. This mechanism — transient bacteremia — is the biological bridge that connects periodontal disease to systemic conditions ranging from endocarditis to adverse pregnancy outcomes.

The dentino-enamel junction (DEJ) is the interface where enamel meets dentin — and it is one of the most remarkable examples of biological structural engineering in the human body. Under microscopic examination, the DEJ is not a flat line but a deeply scalloped, wave-like boundary where rounded protrusions of dentin interlock with corresponding concavities in the overlying enamel. This scalloped architecture prevents fractures originating in the enamel from propagating catastrophically into the dentin and pulp.

Cementum is the thin, mineralized tissue covering the root surface of every tooth — and it is arguably the least appreciated component of the tooth-supporting apparatus. Without cementum, the periodontal ligament fibers that suspend the tooth in its bony socket would have nothing to attach to, and the tooth would simply fall out. This bone-like tissue, only 50 to 200 micrometers thick, serves as the critical interface between dentin and periodontium.

Caries is a multifactorial disease, and sugar consumption is only one of many variables. Some individuals — estimated at 5 to 10 percent of the population — remain caries-free despite high sugar intake, a phenomenon known as the 'caries-resistant phenotype.' This resistance is not due to a single factor, but to a constellation of protective traits: higher enamel microhardness, superior salivary buffering capacity, a non-cariogenic oral microbiome, and tooth morphology that promotes self-cleansing.

Gingival recession affects up to 88 percent of adults over age 65, and one of its primary preventable causes is over-brushing with excessive force. AI-powered electric toothbrushes equipped with pressure sensors, inertial measurement units, and real-time machine learning algorithms can detect when brushing force exceeds safe thresholds and intervene instantly via haptic feedback before the cumulative damage to the gingival margin becomes permanent.

Older adults with arthritis face a double burden: the same manual dexterity limitations that make thorough toothbrushing difficult also increase the risk of periodontal disease, root caries, and tooth loss. Traditional oral hygiene instruction has a dismal long-term adherence rate in this population, with 70 percent of older adults abandoning proper technique within three months. AI-powered brushing coaching systems provide real-time, personalized, adaptive guidance that compensates for dexterity limitations and reinforces correct technique on every single brushing occasion.
Электрическая зубная щетка BrushO с ИИ дает подсказки в реальном времени, обратную связь по давлению, отслеживание покрытия и отчеты о прогрессе в приложении для более чистой ежедневной рутины.
Электрическая зубная щетка BrushO с ИИ дает подсказки в реальном времени, обратную связь по давлению, отслеживание покрытия и отчеты о прогрессе в приложении для более чистой ежедневной рутины.
Address: RM 1427, 14/F RADIO CITY 505, HENNESSY RD CAUSEWAY BAY, HONG KONG
Code: 000000
Phone: +852-53758652
Email: customerservice@brusho.com